Case Introduction
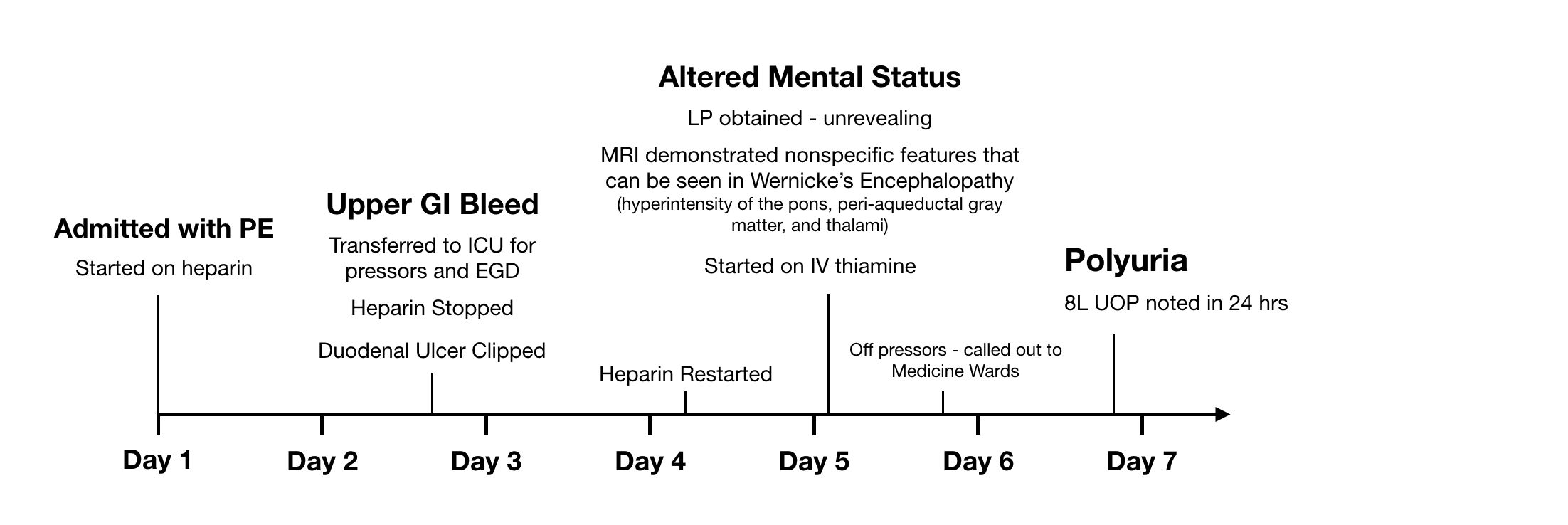
The patient is a 74 year old man with a history of COPD (not on O2), DM2 (not on insulin), Lung Cancer (stage 1 SCC s/p resection 1 year prior), BPH, and cognitive impairment who presented with a pulmonary embolism. Upon initiation of anticoagulation with heparin, he developed a hemodynamically significant upper GI bleed, found to have a duodenal ulcer on EGD s/p clipping. He briefly required pressors in the ICU in the context of this hemorrhage. His ICU course was further complicated by altered mental status (worse than baseline cognitive impairment), presumed to be caused by Wernickes encephalopathy from malnutrition (no h/o EtOH use). Upon transfer from ICU to medicine floor, the patient was noted to have 8L of urine output in 24 hours. Why has he developed polyuria? And how will we manage this?
PMH
Dementia
COPD (not on O2)
DM2 (not on insulin)
BPH
Lung SCC s/p resection
Meds
Pantoprazole
Heparin Drip
Thiamine
Melatonin
Exam
T 97.8F | BP 122/74 | HR 84 | SpO2 98% on ambient air
GENERAL: Sitting comfortably in bed. NAD.
HEENT: No JVD. MM dry.
PULM: Clear lungs throughout.
COR: RRR, no m/r/g.
ABDM: Soft, non-tender, non-distended.
EXTR: WWP, bilateral LE pitting edema 1+
NEURO: Alert, conversant. Oriented to place but generally confused. Occular exam w/ vertical nystagmus and bilateral impairment in abduction. CNs otherwise intact. Strength intact throughout. Normal reflexes.
24 Hour I/Os
Inputs
2.0L LR
550cc water (PO)
Outputs
6.5L Urine
LAB VALUES
Chem.
Na 142
K 3.5
Cl 109
Bicarb 26
BUN 3
Cr 0.5
Gl 196
Ca 8.4
Mg 2.1
Phos 3.6
Alb 2.2
Tbili 0.2
ALT 25
AST 21
AlkP 46
Hem.
WBC 5.2
Hgb 9.5
Plt 188
Question 1:
Based on this initial information alone, what are some possible causes of the patient's polyuria?
Question 2:
What additional diagnostics would you send?
Initial Urine Chemistries:
Urine Osm 322
Urine Na pending
Urine K pending
No Glucose on Urine Dipstick
Question 3:
How does the UOsm value affect your DDx?
After the initial urine chemistries below returned, the patient received ddAVP.
Repeat urine studies are obtained 24 hours later:
Initial Urine Chem.
Osm 322
Na 146
K 11
Initial 24 Hr Urine Output
6.5L
Repeat Urine Chem.
Osm 534
Na 223
K 31
Urea 58
Subsequent 24 Hr Urine Output
4.0L
Question 4:
What is the most likely cause of the polyuria at this point?
Question 5:
Would you have administered ddAVP? Why or why not?
Revisit the case after reviewing background, concepts, and frameworks
Additional Upcoming Questions:
What is the specific etiology of this naturesis?
How can we exclude a superimposed water diuresis?
How will this polyuria affect the patient's volume status and osmolarity?
How do we manage this case of polyuria?